The scientific evidence I’ve studied on lockdowns suggests they don’t work. The places with the highest death rates all had them
The history of medical interventions tells us that often the accepted way of doing things turns out to be dreadfully wrong. I fear this is going to be the case with this so-called Covid ‘cure’.
“Paradoxically, human beings, when compelled to act, learn to justify a chosen course with an assurance unwarranted by the evidence for the course chosen.” – Bernard Lown.
I have studied the history of medicine, and medical interventions, for many years. The most extreme disasters have always followed a fairly distinct pattern. A series of steps, if you like.
Step one: We have a serious disease that is killing lots of people.
Step two: It creates great fear, and the medical profession has nothing much in place to deal with it.
Step three: A charismatic leader emerges to decree that he (almost always a ‘he’ up to now) knows how to treat it/control it, etc. This is ‘the idea’.
Step four: The ‘idea’ is enthusiastically taken up around the world and becomes mainstream thinking.
Step five: The ‘idea’ becomes standard practice.
Step six: The ‘idea’ is taught to medics and becomes accepted truth, a fact.
Step seven: Anyone who goes against the ‘idea’ is ruthlessly attacked.

There is always, of course, the possibility that the ‘idea’ is the best thing to do. This happens from time to time. However, there seems to be little or no correlation between the enthusiasm – and speed – with which ideas are taken up, and the likelihood that they are correct.
The problem, as I came to recognise, lies between step two and step four. By which I mean that a charismatic figure convinces everyone that they have the answer, before there is any evidence to support it. The person may not be charismatic, rather simply someone who has the ability to grab attention and push the ‘idea’ forward. Such as the Chinese premier.
Another thing that leads to disaster, which is of perhaps even greater importance, is that the ‘idea’ must sound like the most obvious common sense. It should trigger a response along the lines of “Yes, of course, that sounds perfectly reasonable.” Once that’s been achieved, the ‘idea’ drops neatly into people’s minds, settles down, and grows roots, creating not a ripple of cognitive dissonance.
At which point it cements itself in, and becomes difficult – even painful – to remove.
To quote the film ‘Inception’: “What is the most resilient parasite? Bacteria? A virus? An intestinal worm? An idea. Resilient... highly contagious. Once an idea has taken hold of the brain it's almost impossible to eradicate. An idea that is fully formed – fully understood – that sticks; right in there somewhere.”
We love ideas; they make us who we are. We defend them, sometimes with our very lives.
“Why do people insist on defending their ideas and opinions with such ferocity, as if defending honour itself? What could be easier to change than an idea?” – JG Farrell.
So, yes, I have no illusions about the strength of ideas. They are so powerful, and so dangerous, that you must be very careful where you aim them. Because ideas also have a God-like power, which is that they are immortal.
Also on rt.com The UK’s vaunted NHS is a National Health Shambles – it wasn’t ready for the Covid second wave and can’t cope. What a surpriseThe damage inflicted by medical ideas
You can kill a person who holds an idea. You can kill thousands of people who hold the same idea – but you cannot kill that idea. Unless you kill every single person who believes in it, then wipe it from the historical record, so that no-one can ever think it again. See ‘1984’.
I will give you a couple of examples of horribly damaging medical ideas. The first is the radical mastectomy. An idea first driven by William Halsted, a US surgeon from the end of the nineteenth century. He believed, as did almost everyone else at the time, that breast cancer spread locally – as did all cancers. Therefore, anything located anywhere near the cancer had to be cut away in case it had already been polluted.
With a radical mastectomy the entire breast, the other breast, muscles on the chest wall, lymph nodes, more muscles were cut out. Almost anything that could be removed without actually killing the women in the process.
The mutilated women were immensely grateful, and the surgeons proud of their expertise. They were doing a good thing, because the idea was considered to be inarguably correct. Questioning it was to be met with the response like, ‘Do you want these women to die – you heartless swine?’

Except that it wasn’t correct. Breast cancer does not spread locally. At least, when it does, it does so very slowly. The spread that causes problems, and kills women, is not local. Cancer cells get into the lymphatic system, and the bloodstream, and spread widely around the body, very early on. Often, long before the primary cancer can be detected.
Those who questioned the radical mastectomy, were attacked. Geoffrey Keynes, brother of John Maynard, tried less radical surgery in the 1920s. It did not go down well:
“Halsted’s followers in America ridiculed this approach, and came up with the name ‘lumpectomy’ to call the local surgery. In their minds, the surgeon was simply removing ‘just’ a lump, and this did not make much sense. They were aligning themselves with the paradigm of Radical Mastectomy. In fact, some of the surgeons even went further to come up with ‘superradical’ and ‘ultraradical’ procedures that were morbidly disfiguring procedures where the breast, underlying muscles, axillary nodes, the chest wall, and occasionally the ribs, part of the sternum, the clavicle and the lymph nodes inside the chest were removed. The idea of ‘more was better’ became prevalent.”
More is better… this is another of the deadly repeating themes of ‘the idea’. The idea can never be wrong, it is just that people are not doing it with sufficient vigour. If women are still dying from metastatic breast cancer, even after radical mastectomies (and they were), the answer could not possibly be that the procedure doesn’t work. The answer is that we are not being radical enough: “Hack away more, and then more.”
Also on rt.com As a doctor, I’ve studied the data swirling around this perplexing Covid virus. One stark truth stands out: lockdowns don’t work‘I was greeted with hands stretched out in a Nazi salute’
Another big medical idea is that of bed rest following a heart attack. It was thought, at one time, that all heart attacks were fatal. James Herrick, another US doctor, described the first non-fatal heart attack in 1912, then suggested that following such an attack, strict bed rest was important. This would take pressure off the heart and allow it a chance to heal. Again, this sounds perfectly reasonable. As described by Dr Bernard Lown, a professor of cardiology and the developer of the defibrillator:
“To a medical novice like me, the justification for enforced bed rest was persuasive. It was based on a sacrosanct therapeutic principle, the need to rest a diseased body part, be it a fractured limb or a tuberculosis-affected lung. Unlike a broken bone, which could be immobilized in a cast, or a lung lobe, which could be collapsed by inflating the chest cavity with air, the heart could not be cradled into quietude. The only approximation for a diseased heart was to diminish its workload. It was long known that during recumbency the heart rate slows and blood pressure drops, both indices of less oxygen usage and therefore of decreased cardiac work. Heart rest was therefore equated with bed rest.”
And so it became standard practice. It was simply what you did:

“Patients were confined to strict bed rest for four to six weeks. Sitting in a chair was prohibited. They were not allowed to turn from side to side without assistance. During the first week, they were fed. Moving their bowels and urinating required a bedpan. For the constipated, which included nearly every patient, precariously balancing on a bedpan was agonizing as well as embarrassing.
“Because world events might provoke unease, some physicians prohibited their patients from listening to the radio or reading a newspaper. Visits by family members were limited. Since recumbency provoked much restiveness and anxiety, patients required heavy sedation, which contributed to a pervasive sense of hopelessness and depression. Around one in three patients died.”
Bed rest started as a relatively mild thing. However, as it is with almost all things, it became increasingly ‘radical’. Lown, along with his mentor Dr Samuel Levine, tried to change this. He became involved in trying to get patients up out of bed to sit in a chair:
“Little did I realize that violating firmly held traditions can raise a tsunami of opposition. The idea of moving critically ill patients into a chair was regarded as off‑the‑wall. Initially the house staff refused to cooperate and strenuously resisted getting patients out of bed. They accused me of planning to commit crimes not unlike those of the heinous Nazi experimentations in concentration camps. Arriving on the medical ward one morning I was greeted by interns and residents lined up with hands stretched out in a Nazi salute and a ‘Heil Hitler!’ shouted in unison.”
Step six: Anyone who goes against the ‘idea’ is ruthlessly attacked.
Also on rt.com The risks of ‘long Covid’ are devastating, especially to those with underlying health problems – it’s killing thousandsNo evidence, no problem
Then, among all the other problems with ‘the idea’, between steps two and three, is one that I have not yet mentioned. It is that no study is ever done to find out whether or not the idea works. It is just conceived to be so obviously beneficial, such common sense, that there would be no point in wasting time and resources trying to prove that it worked.
No-one ever did a study to find out if the radical mastectomy improved survival. No-one ever did a study to prove that bed rest saved lives. They were both introduced on the back of absolutely nothing. In time, eventually, the folly of both was finally recognised. It took 70 years for radical mastectomy, 50 for bed rest.
Which takes us to lockdowns. The most expensive, invasive, and potentially destructive medical intervention ever attempted by humanity. Was there any evidence from anywhere, before we embarked upon them, that lockdowns would work? No, there was none. But we have the six steps on full display here.
Step one: We have a serious disease that is killing lots of people – check.
Step two: It creates great fear, and the medical profession has nothing in place to deal with it – check.
Step three: A charismatic leader emerges to decree that he (almost always a ‘he’ up to now) knows how to treat it/control it etc. This is the ‘idea’ – check.
Step four: The ‘idea’ is enthusiastically taken up around the world and becomes ‘mainstream thinking’ – check.
Step five: The ‘idea’ becomes standard practice – check.
Step six: The ‘idea’ is taught to medics and becomes accepted truth, a fact – check.
Step seven: Anyone who goes against the ‘idea’ is ruthlessly attacked – check.
Does it work? Have lockdowns worked? You can pick and choose countries to support the case that it does and dismiss any evidence you don’t much like. Unfortunately, once you introduce a medical intervention that affects everyone, everywhere, you have lost the possibility of carrying out a controlled experiment of any sort.
Despite the lack of any randomised evidence, most people are absolutely convinced that lockdowns work to control the spread of Covid-19. They point to various countries, e.g. New Zealand, Norway, Australia and Taiwan, to prove their case. They always have a ready explanation as to why countries that underwent lockdown still have high death rates and vice-versa.
The ‘idea’ has become the truth. Its proponents now demand that those who doubt the efficacy of lockdowns prove that they don’t work. It is not the job of those suggesting lockdowns don’t work to prove that they don’t, it is the job of those promoting them to prove that they do.
The starting point for any scientific hypothesis is for the proponents to disprove the null hypothesis. Demanding that those who believe something may not work prove that it doesn’t is to turn the scientific method upside down. You can never prove a negative.
The null hypothesis, by the way, is that there is no difference between two things. Randomised Controlled Trials (RCTs) in medicine are designed to prove, statistically, that there is an actual difference between doing A and B. This is how science is done, how research is done.
Also on rt.com I’m as sceptical as anyone about the government’s narrative on this Covid crisis & the media hype. But 2020 WAS a deadly yearWe must look carefully at the death rates
Unfortunately, it is not possible to do a controlled trial with Covid-19. The possibility of doing any randomised study was lost very early on. Which means that we are instead forced to rely on observational studies. We can look at country X, that did Y, and see how it compares with country Z that did not do Y.
Or we can look at two countries that did Y, to see how they compare. Or two countries that did not do Y. With Covid, of course, no two countries did exactly the same thing. Not even the four ‘countries’ within the UK. So any observations become more difficult to rely on due to this ‘confounding variable’.
In some UK countries, six people could meet up, while in others it was eight, or two households, or only one household etc. In some, restaurants were open, in others they were shut – at varying times. From a scientific perspective, it’s a mess.
Anyway, to simplify things, let’s look at the 10 countries around the world with the highest death rate from Covid. That is, deaths per million population (I have left out countries with a population of less than one million, such as Monaco, or Liechtenstein, because a few deaths here or there can distort the death rate considerably)
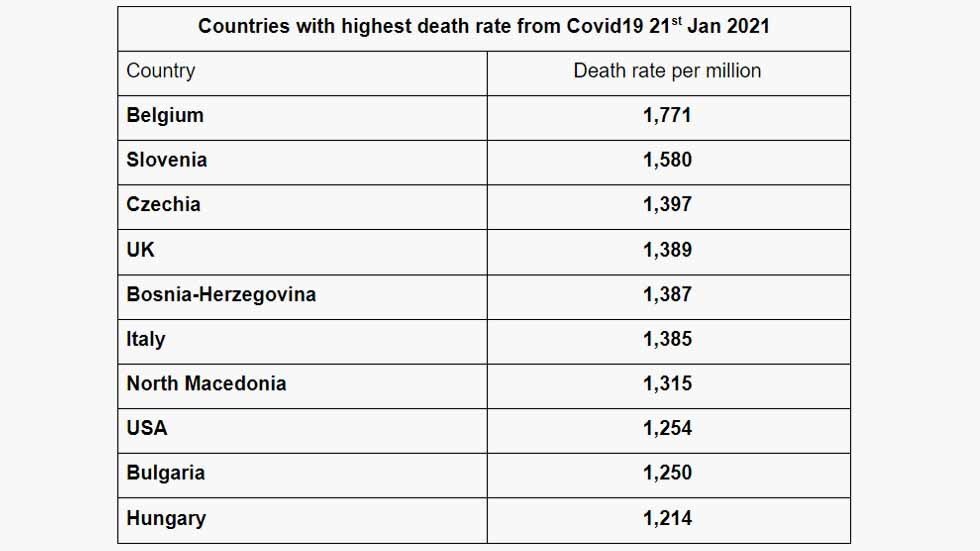
What did they do differently, and what did they do the same? These countries all locked down, relaxed them, then brought in tighter lockdowns at various times. Looking only at first lockdown dates:
Belgium first locked down on March 18, 2020.
Slovenia first locked down on March 20, 2020.
Czechia first locked down on March 16, 2020.
The UK first locked down March 23, 2020.
Bosnia-Herzegovina first locked down March 16, 2020.
Italy first locked down March 9, 2020.
North Macedonia first locked down March 18, 2020.
The USA is highly federal and different states took different approaches – seven states did not issue lockdown orders: Arkansas, Iowa, Nebraska, North and South Dakota, Utah, and Wyoming. In those seven states, the death rate from Covid averaged at 1,280 per million, versus 1,254 as the US average.
In comparison, New Jersey first locked down on March 21, 2020, and its current death rate is 2,310 per million. New York locked down on March 12 – its current death rate is 2,130 per million. These states have the highest Covid related deaths in the US.
Bulgaria first locked down on March 13, 2020.
Hungary first locked down on March 28, 2020.
All countries locked down, Italy first, Hungary last. As you can see, the date of first lockdown is unrelated to the death rate. The other stand-out facts are that these are all countries with majority Caucasian populations. They are all in the northern hemisphere.
People will say, ah, but what about variables, such was population density, age distribution, number of tests done… etc, etc (there are dozens to choose from)? In the end, you can only rely on two things – did a country lock down and what is the death rate from Covid? These are the inescapable facts, everything else can be twisted to suit any argument.
If I were thinking of running a clinical trial where the hypothesis was that a lockdown was the best way to prevent deaths from Covid, then I would start by looking at observational data such as this.
I would find that the 10 countries in the world with the highest death rates all locked down.
I would look at the US, where the death rates in states that locked down, and those that did not, were almost the same rate (or vastly higher in the cases of New Jersey and New York), and I would conclude that the observational studies had – thus far – failed to disprove the null hypothesis. In fact, the evidence up to this point could suggest that lockdowns may actually increase the death rate.
In short, I would look for another idea.
Think your friends would be interested? Share this story!
The statements, views and opinions expressed in this column are solely those of the author and do not necessarily represent those of RT.